




UNESCO | Bringing living heritage in Nepal’s schools-a new beginning in innovative teaching and learning

UNESCO works to attain quality education for all, focusing on women empowerment and literacy, to rehabilitate cultural heritage after the earthquake, promote cultural diversity and intercultural dialogue, to mobilize scientific knowledge, to promote press freedom, freedom of expression, media development and to advocate for the rights and safety of journalists.
In Culture sector, the Office is committed to strengthen the role of culture as enabler and driver of sustainable development, through its support to Nepal in promotion, protection, conservation and safeguarding of country’s unique tangible and intangible heritage by increasing the people’s awareness and strengthening national capacities at all levels.
![]()
Intangible Cultural Heritage – or ‘living heritage’ – is inherited from ancestors and passed on to descendants. It includes oral traditions, performing arts, social practices, rituals and festive events, knowledge and practices concerning nature and the universe, and the knowledge and skills, that are meaningful to the communities. It is continuously recreated as it is transmitted from generation to generation and evolves in response to our environment. Living heritage is important because it offers communities and individuals a sense of identity and continuity. Living heritage contains locally rooted knowledge and provides a source of resilience against changing climatic conditions as well as at time of emergencies. It promotes social cohesion, respect for cultural diversity and human creativity, as well as help communities building peaceful and inclusive societies.
As the United Nations specialized agency for culture, UNESCO is tasked with safeguarding living heritage and ensuring its transmission to future generations. The 2003 UNESCO Convention for the Safeguarding of the Intangible Cultural Heritage encourages and supports countries to take the necessary measures to ensure that communities can safeguard their living heritage.
Safeguarding living heritage is important to address some of the most significant challenges of today and build inclusive, resilient, and sustainable societies for the future. However, the localized system and traditional mode of intergenerational transmission of living heritage, which is a dynamic interactive process, is often at risk and/or disrupted due to various reasons such as rapid urbanization, natural or manmade disaster, displacement, out-migration, globalization, the advent of the digital age and many more.
Education plays a key role in safeguarding intangible cultural heritage. The 2003 Convention recognizes the transmission of intangible cultural heritage ‘through formal and non-formal education’ as a key safeguarding measure. The Convention calls on States Parties to ensure recognition of, respect for, and enhancement of intangible cultural heritage through education programmes. These can include:
- programmes in formal learning environments such as in primary, secondary and post-secondary schools.
- non-formal opportunities such as short courses, community learning and capacity-building activities.
Experiences have shown that teaching core subjects such as mathematics, science, or literature by using students’ cultural backgrounds can make the learning process more relevant, as it creates better connections between what is taught in classrooms and the children’s everyday life and their surroundings. This also allows students to explore their identity, learn to respect cultural diversity and reflect on their heritage and that of others and help find local solutions to global problems related to climate change, health, etc.
Since the heritage bearers – the communities and groups concerned- are at the heart of safeguarding living heritage, reconnecting school (youth) with communities provides the opportunity for survival into the future. This can provide rich resources as well as context-specific content and pedagogy for education programmes, thus act as leverage to improve the relevance of education and learning outcomes. In the meantime, this opportunity can help safeguard intangible heritage through education. For example, education for sustainable development uses indigenous knowledge and skills as a key resource for communities in understanding the environment, sustainably using its resources, assessing climate change impacts, and adapting to them. This linkage also promotes cross-sectoral and multi-level cooperation among diverse stakeholders. Therefore, UNESCO promotes learning and teaching through and about ICH in education programmes in all relevant disciplines.
Approaches to bring intangible cultural heritage into classrooms and non-formal education spaces can vary depending on the local context, needs and educational level.

Good Neighbors International | COVID-19 Response
Since April 2020, GNI Nepal has been supporting the central, provincial, and local governments across Humla, Mugu, Darchula, Bajura, Doti, Kailali, Bardiya, Myagdi, Kaski, Parbat, Nawalparasi East, Nawalparasi West, Gorkha, Nuwakot, Kathmandu, Lalitpur, Morang, Jhapa and Panchthar districts with essential medical equipment, food and non-food items, health,WASH and education interventions.
In 2020 and 2021, GNI Nepal reached 17,150 food-insecure households with food and livelihood support, 1.2 million rural children with radio schooling program, central and local governments with medical equipment, non-food items and cash support, and communities with public service announcements and radio shows to raise awareness of COVID 19, child protection, education and public health-related issues. GNI Nepal has so far invested NRs. 157,968,805 in supporting the communities and Government of Nepal in combating COVID-19. The pandemic will continue to impact communities into the foreseeable future, GNI Nepal will continue response and recovery interventions as per need.

Health and WASH
GNI Nepal provided 34,140 RT-PCR kits, 30,167 RNA extraction kits, 19,850 VTM swab collection kits, 46,762 surgical masks, 2,700 KN95 masks and 5,455 PPE sets, 20,500 pairs of sterile gloves, 1,200 goggles, 65 infrared thermometers to the Government of Nepal. Additionally 14, 281 antigen kits, 395 bottles of disinfectants, 67 finger pulse oximeter, 26 ICU material sets, medical equipment for 13 health posts, 15 nebulization machines, 13 oxygen concentrator, 15 oxygen cylinder, 785 oxygen flow meter, 1,135 oxygen mask, 457 oximeters, 1,410 reservoir bag masks, and 10 ventilators were also provided to local, provincial, and federal governments.
350 bottles of hand sanitizers, 7,500 bottles of hand wash and 20,868 hygiene kits were provided to health facilities and children in 12 districts respectively. 14 local governments received support for quarantine management and installing 102 handwashing stations.
Holding center for fighting a crisis
Ward No. 5, Mahakali Municipality, Darchula District
In March 2020, Government of Nepal enforced a nationwide lockdown to respond to the crisis. It is estimated that more than one million Nepalis live and work in India. Due to the restriction, thousands of homebound migrant workers were stranded at the Nepal-India border. They lacked access to basic personal hygiene materials and facilities, and medical care.
To support the efforts of the Government of Nepal at containing the virus and managing the humanitarian crisis, GNI Nepal helped establish a holding center at Ghaat Bazaar of Mahakali Municipality, installed a handwashing station at the Nepal-India border, and provided personal hygiene materials. More than 400 incoming and outgoing travelers benefited from facilities and hygiene materials.
Education
The COVID-19 pandemic resulted in countrywide school closures leaving more than eight million children in a limbo for almost an entire year. To address the critical learning gap children were facing, GNI Nepal with technical assistance from the Center for Education and Human Resource Development (CEHRD) and in coordination with Nepal Education Cluster designed and launched Radio Kaksha, Sundai Sikdai, a radio schooling initiative for sixth, seventh, and eighth graders. These classes aired six days a week via Radio Kantipur and re-aired via local radio stations from June to December 2020.
Radio Kaksha reached an approximate 1.2 million learners in 59 districts across the country. Additionally, 3,400 grade ten students of Bajura benefited from Radio SEE Preparation Class, 5889 students benefitted from 172 radio phone-in shows, and 1449 students participated in 75 community-based learning sessions. GNI Nepal also took the lead and contributed to the development of self-learning materials for grades two, three, and five jointly with the Ministry of Education, Science and Technology and Center for Education and Human Resource Development.
As schools have not yet reopened, this year too, the radio program is being rebroadcast across 12 working districts. Furthermore, GNI Nepal is reaching young learners with awareness-raising, psychosocial, learning pack, and home-and community-based learning supports across 11 districts.
Continuing education at home with Radio Kaksha
Prerana Chanda, Grade 8
Janata Basic School
Ward No. 9, Janaki Rural Municipality, Kailali District
Prerana had just finished her seventh-grade final exam in March 2020, when the COVID-19 lockdown took effect. She did not have much to do as she remained at home most of the time. Like every other underprivileged student, she had no access to guided learning. To help students like Prerana, GNI Nepal started airing a radio schooling program which Malika FM, a local radio station also broadcast. Classes for grade six to eight students on three core subjects: English, Science and Social Studies were offered six days a week in the mornings and evenings.
Prerana was fascinated by the newfound source of learning. She could learn just by listening to the teachers speak on the radio. She listened to the classes regularly from the comfort and safety of her home, and enjoyed them as well. Keshav Tamata, Principal of Shree Amarawati Basic School claims, “The radio program was a big hit among local students and they all benefited from it.”
Livelihood
The pandemic has adversely affected the livelihoods of informal sector workers and low-income households. More than one-third of such workers lost their jobs and those employed also had to accept pay cuts. Across 19 districts, GNI Nepal provided NRs. 7,235,855 (62,333 USD) to 37 local governments for helping 17,150 food-insecure households with groceries, smallholder farmers with seeds, and agriculture input support and local business promotion opportunities targeted youths.
With GNI Nepal’s support, 4593 farmers in Lalitpur, Gorkha, Kaski, Parbat, Myagdi, Bardiya, Doti, and Mugu received seeds; 553 farmers received cash for business start-up in Humla, Gorkha, Bajura, Darchula, Doti, and Lalitpur; received groceries; 986 farmers in Bardiya and Kailali received fertilizer; local women made 14,100 masks after participating in a mask-making training. An additional 900 individuals will receive livestock and veterinary services and business skills, conditional cash, and livelihood support.
Making masks, making money
Ward No. 5, Sunwal Municipality, Nawalparasi West District
At the start of the nationwide lockdown, masks were not easily available in Nawalparasi East and West districts because nobody used them. Overnight, it became a vital need and the demand skyrocketed. During the lockdown many people became jobless and also got stuck in their homes. Realizing an employment potential and solution to an emerging demand, 20 local women of Ward No. 5, Sunwal Municipality were provided a one-on-one mask-making training under GNI Nepal’s Inclusive Rural Development Project.
They produced 14,100 masks which contributed to partially meeting the local demand. Each of the trainee mask-maker got NRs. 15 (0.13 USD) for a mask. On an average, they earned NRs. 10,575 (91 USD) for 705 masks, working for 17 days. The ready-to-use masks were distributed among the project’s 6,000 direct beneficiaries and 13 wards of Nawalaparasi East and Nawalaparasi West.
About GNI Nepal
Good Neighbors International (GNI) is an international development and humanitarian organization that empowers people in 40 countries across the world through social development activities and places particular emphasis on their economic development. Good Neighbors International (GNI) Nepal has been working in Nepal since 2002 for improving the lives of poor people, especially children through child protection, education, income generation, health services, water, sanitation and hygiene, disaster risk reduction, and advocacy programs. Currently, GNI Nepal serves marginalized, vulnerable, and poor children, families, and communities in 19 districts across Nepal.
For more information:
Website: www.gninepal.org
Facebook: www.facebook.com/gninepal.org
Instagram: www.instagram.com/gninepal
YouTube: www.youtube.com/gninepal
LinkedIn: www.linkedin.com/in/gni-nepal/
Twitter: https://twitter.com/GNI_Nepal
TikTok: www.tiktok.com/@gninepal
_20210824232942.jpg )
WaterAid Nepal | WASH improvement at health center helps everyone
Water, Sanitation and Hygiene (WASH) in Health Care Facilities (HCFs) is fundamental to improve the safety and quality of healthcare services. Safe dignified care relies on clean water, decent toilets and good hygiene, all of which must be underpinned by a strong and resilient health system. Better WASH services result in fewer healthcare related infections, an increase in use of health services, improvement in staff performance and morale and build them as a role model for the community to set community hygiene norms. Adequately equipped healthcare facilities are vital in treating patients and advising them on good hygiene to control the spread of COVID-19 and tackle future pandemics and other health crisis.
Nonetheless, WASH in Healthcare Facilities is often a neglected crisis. Instead of being models of good WASH practices, HCFs suffer from water shortages, poor water quality, deteriorating water infrastructure, lack of water storage tanks, insufficient sanitation blocks in poor state of operation, not inclusive and user-friendly, poor hygiene conditions etc. Drawing from World Health Organization’s (WHO) report on the assessment of WASH in healthcare facilities in 54 low and middle-income countries published in 2015, representing 66,101 facilities show that, 38% lacked an improved water supply, 19% did not have improved sanitation and 35% had no soap and water for hand washing. This lack of services compromises the ability to provide basic, routine services, such as child delivery and compromises the ability to prevent and control infections.
In Nepal, the situation in Healthcare Facilities is dismal where 36% of Healthcare Facilities do not have basic water supply, 8% of HCFs still do not have toilet facilities, only 46% of HCFs have handwashing materials at point of care, and just 1% of HCFs have basic waste management practices (JMP Baseline 2019).
Adequate and inclusive water, sanitation and hygiene conditions and practices in the healthcare facilities are the prerequisites to providing high-quality health care services. With the growing number of deliveries taking place in the birthing centres, these WASH conditions and practices (at least basic level as defined by WHO-UNICEF-JMP WASH service level for HCF and The National Standards for WASH in HCF, draft 2018) within healthcare facilities must be improved in order to achieve national and global Sustainable Development Goal (SDG) targets.
In 2019, a World Health Assembly Resolution on WASH in health care facilities, agreed to by 194 member states, outlined concrete actions that countries can commit to. These included establishing national roadmaps and targets, implementing standards, integrating WASH and IPC indicators into health programming and monitoring and increasing domestic funding.
The healthy start project
|
In the past three years, WaterAid Nepal (WAN) reached:
|
WaterAid Nepal (WAN) implemented The Healthy Start project (HSP): WASH in Healthcare Facilities (HCFs) in Bardiya district from 2018-2021 with an aim to improve water, sanitation and hygiene services in Healthcare Facilities and also contribute to reduction of neonatal mortality. The Healthy Start enabled Health workers and Pregnant and Lactating Mothers (PLMs) to have access to safe water and improved sanitation facilities in the birthing centers of 8 HCFs out of the 34 HCFs in the district. The three-year long project, anchored by WAN’s programmatic approach of “Doing some and influencing the rest”, was implemented by WaterAid Nepal (WAN) in partnership with Backward Society Education (BASE).
_20210824232921.jpg)
Key focus of the project in transforming the lives of the Healthcare Workers
Model WASH facilities sanitation, and hygiene facilities in the selected HCFs. These WASH facilities were built as per the National standards for WASH in HCFs-Draft 2018, with an aim to support the local governments to learn and replicate such model of WASH invention throughout the district.
National standards on Water, Sanitation and Hygiene in Health Care Facilities has tried to capture the basic and advance service level of water, sanitation and hygiene according to the SDG.
As per the baseline survey conducted in November 2018, only 32% of HCFs had the availability of an alternative improved source of water. Only 32% HCFs had separate toilets for males and females and the percentage of HCFs with at least one usable improved toilet that meets the needs of people with reduced mobility was only 3%. Only 9% HCFs met the criteria for ‘Basic service level’ for hygiene as defined by JMP and only 44% HCFs had cleaning protocols available. Out of 34 HCFs, only 3% met the ‘Basic service level’ standard for waste management.
To cope with the of lack of adequate WASH facilities and to deliver better health services for Pregnant and Lactating Mothers (PLMs) and provide better child care, there was urgent need to construct inclusive WASH facilities to contribute to the decline of health complications often caused by poor WASH services in HCF.
As a follow up to the counselling sessions, hygiene promotion sessions at the community level were organised to reiterate the hygiene behaviours. Health and hygiene officers formed several groups of PLMs at the community level where five key hygiene behaviours were promoted using tools like flipchart, storytelling, handwashing rituals, games, commitment-making and certificates for participants.
The hygiene sessions were delivered to a group of 15-20 PLMs at the community level in one-month interval before the pandemic. The number was later reduced to 10 due to COVID-19, but there was a need to double the frequency of such sessions to reach the targeted number of PLMs. COVID-19 preventive messages were also disseminated through distribution of flyers and broadcasting of jingles regularly and frequently through local radio. During the hygiene sessions, “model families” were chosen, who received recognition and appreciation for adopting all the hygiene behaviours. Similarly, another motivational factor contributing to behaviour change was the “healthy mother award” presented to the one mother who diligently followed all the key hygiene behaviours.
The overall hygiene intervention followed the “Behaviour Centred Design” (BCD) approach to hygiene promotion, which was designed in reference to the result of the formative research conducted for hygiene promotion through routine immunization (HPTRI) project.

The hygiene sessions at the community level was followed by monthly household visits by Female Community Health Volunteers (FCHVs) to run the campaign contributed towards improving knowledge on hygiene related behaviours and transcribing it into practice. A total of 936 PLMs was directly reached with hygiene sessions at the community level whereas the secondary data collected from 34 HCFs show that a total of 7,484 ANC visits were recorded indicating that many pregnant mothers received personal counselling sessions during their ANC visits to the HCFs. They might have also received these personal hygiene counselling during their PNC visits after the successful delivery of their new-borns and any other follow-up visits to the HCFs
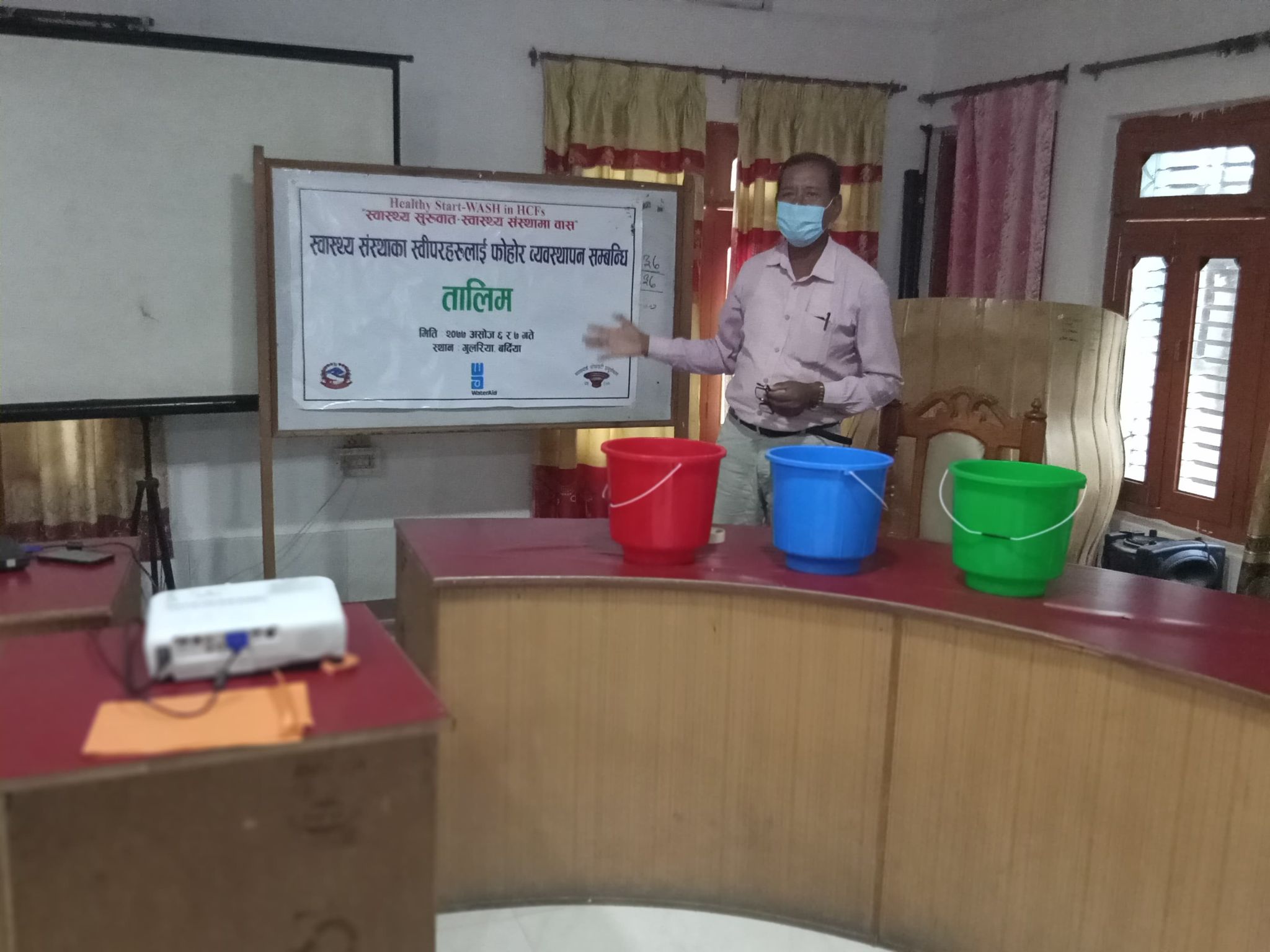
3. Capacity building of healthcare facility staff
Healthy Start project reached over 121 HCF staff which included HCF In-charges, health workers, auxiliary nursing midwives (ANMs), cleaners, health facility operation and management committee (HFOMC) members, health coordinators, etc. with numerous trainings and orientation workshops on the importance of WASH in HCF, personal counselling, Water and Sanitation for Health Facility Improvement Tool (WASH FIT) to assess the WASH status in HCF and accordingly prepare the WASH Improvement Plans.
During the first year of project intervention, several sensitizing orientation and Hygiene training packages were developed based on the scoping assessment carried out from several HCFs. Interviews with respective HCF staff, HFOMC members, other stakeholders including service seekers and observations from the field visits were also undertaken.
The HCF In-charge from all 34 HCFs were trained on WASH in HCF to supervise and monitor the work of health workers and provide onsite coaching to ANMs, specially to conduct personal counselling sessions on hygiene behaviours along with other regular health check-up, advice and guidance. This was followed by a training to the ANMs from all 34 HCFs on WASH in HCF with focus on personal counselling and promoting five key hygiene behaviours using hygiene flipchart.
_20210824233105.jpg)
These trained health workers then provided hygiene sessions to PLMs during ANC/PNC counselling visits. A total of 33 onsite coaching and monitoring events were carried out by respective health coordinators and HCF In-charges providing further practical tips of counselling with demonstration exercises. Since the sanitation workers play a vital role in maintaining good hygiene and good environmental sanitation, a hands-on refresher training on environmental sanitation was conducted for the cleaners, sweepers, helpers, etc.
End-line evaluation of the project completed in March 2021, indicates that there have been significant improvements in the WASH status in the HCFs. It states that 85% of HCFs have cleaning protocols and 85% of the HCF’s cleaning staff have received trainings as per the protocol.
Orientations and hands on training on water quality was organized for the laboratory staff as well. They were trained to use ENPHO field water test kit to test the water quality in their respective HCFs. The trained laboratory staff after this training have now been ensuring the quality of water in their respective HCFs by conducting the water quality testing on a monthly basis and recording them in their laboratory register. Additionally, the HFOMC members along with HCF staff were also oriented on WASH in HCF with a major focus around using WASH FIT as an assessment tool to assess the existing status of WASH facilities in the HCF and accordingly formulate WASH Improvement Plan to upgrade the situation and service level of the WASH facilities.
Similarly, representatives from local governments including health coordinators, deputy (mayors), vice (chairpersons) were sensitized on the importance of WASH in HCF in orientation workshops to highlight the crucial role of WASH in HCF. Few representative ward chairpersons were also included in the orientation sessions along with their respective HCF In-charges. The Mayors and Chairpersons expressed their commitment to advocate and prioritize the agenda of WASH in HCF in their municipal council meetings and accordingly include in the local level strategy, plan, and budget. It is expected that they will incorporate the agenda of WASH in HCF in upcoming local programme plans with respective budget allocation.
_20210824233152.jpg)
4. National level policy influencing through WASH in HCF Technical Working group
A technical working group on WASH in HCF at the Federal level, formed in 2017, in leadership of Ministry of Health and Population (MoHP), Management Division. Multi- sector Coordination Section, Health Coordination Division, Ministry of Water Supply/ Department of Water Supply and Sewerage Management, Curative Division, Epidemiology and Disease Control Division, WHO, UNICEF, USAID, SNV, NSI, PSI, ACF, TDH, Save the Children, WaterAid Nepal are members of this group with WaterAid Nepal providing secretariat support. The working group has contributed to drafting the National Standards for WASH in HCF in the government leadership and followed up repeatedly advocating for its endorsement. As a result, Ministry of Health and Population (MoHP) has endorsed the WASH in Healthcare Facilities National Standard.
Conclusion
The project was successful in bringing about positive changes in the WASH service level of most of the HCFs in Bardiya district and helped improve service delivery and extension of WASH facilities. Many of the outcome indicators showed improved results in the end-line as compared to the baseline from water, sanitation, hygiene, and waste management perspective. Similarly, this project has also contributed to improve the key hygiene behaviours of the targeted pregnant and lactating mothers (PLMs). At the federal level, WAN demonstrated models, strong evidences and learning from practice helped contribute to national policymaking, including the National Standards for WASH in HCF (draft), which once endorsed will shape the roadmap for WASH in HCF in Nepal – guiding both health and WASH sectors for years to come.

Key performance Indicators showing improved results
Drinking water services
The End-line evaluation showed that 77% of HCFs have tested the water quality of the main source, compared to 32% in the baseline survey. End-line indicates that 97% of the HCFs treat drinking water, which has significantly increased compared to 77% in the baseline.
Sanitation facilities
Out of the 33 surveyed HCFs during End-line evaluation, 32% met the ‘Basic Service’ level of sanitation, indicating sanitation services have improved, in comparison to 0% during the baseline. 68% of HCFs fell under the ‘Limited Service’ level as mentioned in JMP. Out of the 33 surveyed HCFs during End-line evaluation, 32% met the ‘Basic Service’ level of sanitation, indicating sanitation services have improved, in comparison to 0% during the baseline. 68% of HCFs fell under the ‘Limited Service’ level as mentioned in JMP. 85% of HCFs have separate toilets for males and females, in comparison to 32% in the baseline
Hygiene
94% of the HCFs had a functional handwashing station available at the selected point of care as compared to 41% in the baseline. 59% of the HCFs had segregated the waste into at least three labelled bins correctly. This percentage has sharply increased compared to 18% in the baseline. Among those HCFs who had correctly segregated the waste, nearly 65% had kept segregated waste in the color-coded buckets as compared to 24% in the baseline. 41% of the HCFs have disabled friendly handwashing stations, as compared to 0% in the baseline. 94% of the HCFs met the criteria for ‘Basic service’ level for hygiene as defined by JMP, which was 9% in the baseline survey. 85% of HCFs have cleaning protocols available, compared to 44% in the baseline and 85% of the HCF’s cleaning staff have received trainings as per the cleaning protocol.
Waste Management
59% of the HCFs had segregated the waste into at least three labelled bins correctly. This percentage has sharply increased compared to 18% in the baseline. Among those HCFs who had correctly segregated the waste, nearly 65% had kept segregated waste in the color-coded buckets as compared to 24% in the baseline.
Success story: WASH – key to long term community
Safe and readily available drinking water and improved sanitation are vital for long term public health and wellbeing. Yet, many healthcare facilities (HCF) lack basic WASH services, leaving them vulnerable to disease and long-term health problems.
Few years ago, Dhadhawar Healthcare Facility (HCF) in Barabardiya Municipality lacked basic WASH services and safe drinking water making the patients vulnerable to diseases. The health facility had only three toilets, which were on the verge of being destroyed due to the road extension construction work. Men, women, patients and staff were all compelled to use the same toilets. With just one water filter for staff, availability of safe drinking water for patients were a major problem.
WaterAid Nepal, with its local partner organization Backward Society Education (BASE), aims to improve the WASH services in HCFs to provide quality health services. Considering the problems in Dhadhawar HCF, Bio-sand filters were installed for safe drinking water and Child, Gender and disabled (CGD) friendly toilets were built. Now, safe drinking water is readily available for all staff and patients, women and men have separate toilets inside the HCF, hygiene is given utmost importance and various orientations were provided to the cleaning staff to keep the HCF clean.

Since the establishment of birthing center in Dhadhawar Healthcare Facility, the patients and visitors have had a lot of problems with water and toilets, but now there is no such problem, the patients, the visitors and all the concerned bodies and the whole staff are very happy.
Health post in-charge Jung Bahadur Chaudhary says, “We were worried about the demolition of the toilet since the local government was not able to provide the budget to the health post for a substitute toilet. We are thankful to BASE and WAN not just for supporting us with child gender and disabled friendly toilets, but also for installing bio sand filters for drinking water.”
Dhalakl Bista , Health worker, says,“When pregnant and lactating mothers visit the health post for ANC and PNC, the health staff not only check their overall health condition, but also give proper counselling to the mother as well as visitors. They teach them the five key hygiene behaviours and also encourage them to be a model family.”

RTI International | Improving children’s skills, boosting local capacity
A two-year (2020-2022) partnership between the Government of Nepal and the US Agency for International Development (USAID), the Early Grade Reading Program II (EGRP II) is helping children across Nepal learn to read with fluency and comprehension-skills that help set them up for success later in life. EGRP II supports evidence-based reading instruction in grades 1-3 in nearly 14,000 schools in 396 municipalities across 38 districts of Nepal, in line with the Government of Nepal’s National Early Grade Reading Program (NEGRP).
Through strengthened policy, practice, and system capacity, EGRP II will make lasting contributions to improving early grade reading for an estimated 450,000 learners. These efforts build on the foundation laid through USAID’s first Early Grade Reading Program (EGRP) in Nepal. Benefitting more than 550,000 learners in two cohorts across 16 NEGRP target districts, EGRP achieved a significant impact in terms of reading gains. In addition to training, ongoing support to teachers, including mentoring and coaching, is essential to ensure that what is learned is being applied in the classroom.

Working with Nepal’s Center for Education and Human Resource Development (CEHRD), EGPR II is helping to revise and roll out a teacher professional support system to operationalize the new curriculum and materials. According to Jodie Fonseca, EGRP II Chief of Party, “These capacity-building activities are part of EGRP II’s comprehensive approach to strengthening educational capacity, curriculum and teaching, and professional support for educators—even in the face of a prolonged Covid-19 pandemic. Over time, these efforts will contribute to stronger reading skills for children in the early primary grades, in line with Nepal’s education goals.”
As the Covid-19 pandemic forced school closures, flexible learning approaches became critical to ensure continuity of learning. In response, EGRP II provided direct support to local education units to implement community—and homebased learning, targeting 16 rural, disadvantaged municipalities in Province 2 that are heavily impacted by Covid-19. These interventions include small grants to 119 schools, teacher training on flexible learning approaches, distribution of tablets pre-loaded with offline learning content, and provision of decodable books and stationery packs.
From mid-2021 through early 2022, EGRP II will work with district and local governments to scale up these efforts to 264 additional schools in Province 2, ultimately reaching over 73,000 children. Narayan Krishna Shrestha, Director of Programs of EGRP II, shares, “Irrespective of Covid-19, we have continued working with palika members, teachers, and communities to build their capacity through virtual mediums. Our home learning clusters have provided an important space for children to continue their learning journey despite the closure of physical schools. Our engagement with parents through teacher-parent meetings has helped motivate children towards learning at home.”









